
A growing number of physicians are showing interest in resuscitative endovascular balloon occlusion of the aorta (REBOA). Since REBOA is performed only rarely, gaining expertise in this novel procedure is a practical challenge.
“I first learned about REBOA two years ago,” said Christopher Kinsella, MD, a general surgeon. “After reading a lot about the procedure, I decided it was something I would rather do than ED Thoracotomy. But getting training for REBOA was a challenge. And even after you were trained, there were no good tools for practicing the procedure.”
An experienced model maker, Dr. Kinsella used parts from a hardware store to build a REBOA simulator for his personal use. Positive feedback from colleagues soon convinced him there was real demand for a practical REBOA training solution.
Dr. Kinsella spent a year honing his design and developing a high-quality production process. In 2016 he introduced the Medalus REBOA Task Trainer.
“Trauma surgeons told me they needed three things from a REBOA simulator: They need to train placement, they need to train troubleshooting, and they need it to be really easy to operate,” Dr. Kinsella said. “This simulator delivers all three.”
Realistic scenarios for endovascular hemorrhage control
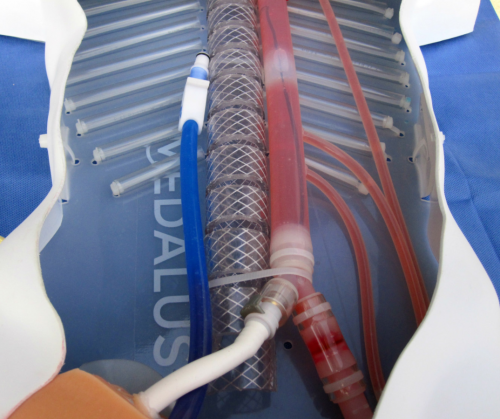
The Medalus REBOA Task Trainer has no electronic parts. Users set up different bleeding scenarios by opening and closing click valves that simulate thoracic, abdominal and pelvic bleeding.
Learning through error. “The trainer is designed specifically to show all the ways in which the procedure can fail,” Dr. Kinsella said. “So you can set up a training scenario in which you basically invite error.”
For example, an instructor could create a simulation for a patient with gunshot wounds to the chest and abdomen. If the learner elects to perform REBOA in this scenario, the mannequin will continue to bleed.
“The system has a Zone 1 bleeding vessel that is impossible to control with REBOA,” Dr. Kinsella said. “So if you inflate the balloon on a ‘chest injury’ patient, the blood level will continue to fall and you will watch the patient bleed out.”
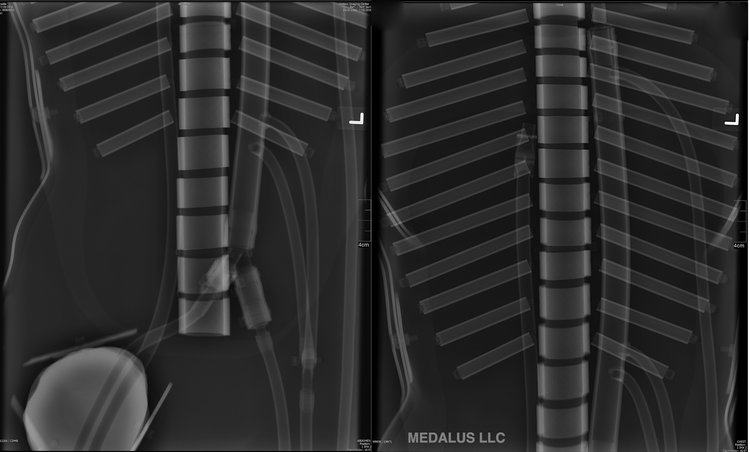
Troubleshooting placement. “The mannequin has a radiographic footprint that correlates with the aortic branches and with the surface anatomy,” Dr. Kinsella said. “So you can place the catheter and then ask for an X-ray or fluoroscopy before you inflate the balloon.”
This allows learners to practice troubleshooting incomplete occlusion and transient patient response. “It also lets you train for Zone 3 occlusion, which is difficult to perform blindly,” he said.
Practicing vascular access. The mannequin’s femoral artery is accurately positioned with reference to surface landmarks. Users feel a slight “pop” upon successful insertion and get an immediate return of pressurized blood flow.
The simulator also includes a femoral vein that can be cannulated, which allows users to practice managing hemorrhage control and resuscitation at the same time.
“Both arteries can be accessed by ultrasound,” Dr. Kinsella said, “which lets you train for high-pressure situations where you are trying to do an insertion on a pulseless, hypotensive patient.”
Fast setup and use, no specialists required
The Medalus REBOA Task Trainer is built without internal step-offs, so guide wires will not get “caught” inside the mannequin. This makes it not only compatible with all balloon catheter systems on the market, but useful for training other endovascular procedures beyond REBOA.
Unlike complex simulation devices, the trainer is easy to maintain and use. Short videos available online provide complete instructions on setting up the mannequin and using it to run multiple REBOA training simulations.
“You don’t have to have a specialist come out and teach you how to use the system or troubleshoot it,” Dr. Kinsella said. “We ship the simulator to a hospital, the trauma surgeons watch a few videos, and they can use it immediately without a hitch.”
To find out more about the Medalus REBOA Task Trainer and access training resources, visit the Medalus website.
