
Physician
Rebecca Vogel, MD, Department of Surgery, St. Anthony Hospital, Lakewood, CO
Presentation
The patient was a 21-year-old female who presented to the Emergency Department after skiing into a tree. She was transported via helicopter after a two-hour extrication off the mountain. The patient became hemodynamically unstable prior to arrival to the ED, was not intubated and presented without a pelvic binder.
Diagnosis
Initial evaluation revealed a right femur and pelvic fractures. Final diagnosis included bilateral pulmonary contusions, left abdominal wall muscular disruption, open book pelvic fracture with pelvic ring instability, sacral fractures, right midshaft femur fracture, right acetabular fracture and left comminuted elbow fracture with posterior dislocation.
Course of care

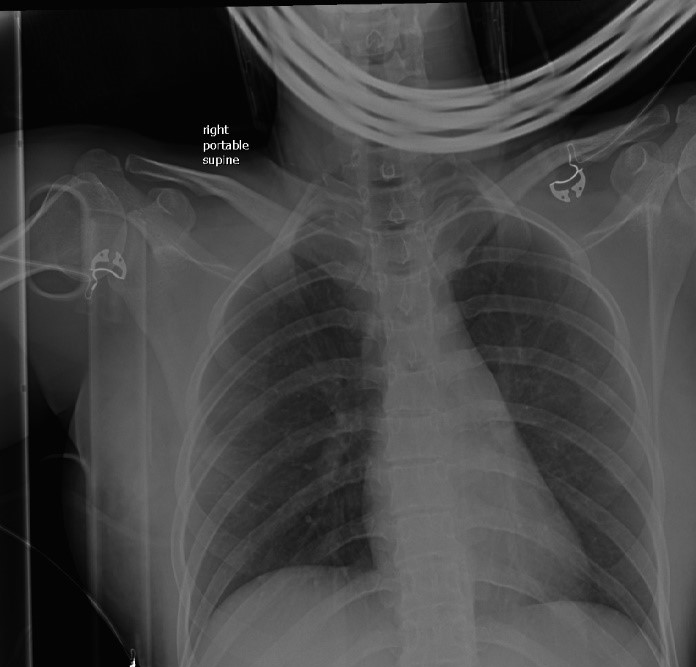
The patient entered the Emergency Department as a highest-level trauma activation. Heart rate was in the 160s with an arterial blood pressure of 48/22. Base deficit and lactate were 12 and 2.1 on admission. Patient was alert and talking despite her profound hypotension. Patient was intubated and central line placed while pelvic binder was applied and FAST was performed. Massive transfusion protocol was initiated. Chest (Figure 1) and pelvic (Figure 2) x-rays were obtained. FAST was negative for any evidence of blood in the peritoneal cavity. CXR revealed no obvious injury, and the pelvic x-ray was positive for an open book fracture.
Due to the patient’s continued hemodynamic instability despite resuscitative efforts, an ER-REBOA™ Catheter was utilized. The initial approach for access via ultrasound to the common femoral artery was on the patient’s left side, as it was opposite the right femur fracture. The initial approach was unsuccessful as the wire was unable to thread into the vessel properly. As a result, the ER-REBOA™ Catheter was placed into the patient’s right side, using ultrasound as guidance for percutaneous access, where the wire was easily passed.

The ER-REBOA™ Catheter was placed into Zone III. The balloon was inflated with 8 cc of a 1:3 ratio of contrast to saline, and placement of catheter was confirmed with x-ray (Figure 3). After balloon inflation, patient’s heart rate came down to the 110s and systolic blood pressure went up to the 90s. A total of 2 units pRBCs and 2 units FFP were transfused.
The patient was taken to CT to rule out head or other solid organ injury while IR was preparing the hybrid OR suite for an angioembolization. Preceding the pelvis portion of the CT scan, the balloon was deflated temporarily, less than two minutes, at the request of IR as a means to identify the area of extravasation. The SBP decreased from the 110s down to 85-90. The balloon was re-inflated after the pelvic CT scan was completed. The balloon was ultimately deflated and the ER-REBOA™ Catheter pulled once IR was prepped and draped. The balloon was inflated for approximately 28 minutes.

IR used the previously placed 7Fr sheath from the Prytime convenience kit for access. The patient’s bilateral hypogastrics were embolized (Figure 4). The sheath was left in for 24 hours to ensure access in the event additional angio was necessary. Patient received 16 units PRBCs, 13 units FFP, 4 (5-packs) cryoprecipitate, and 2 units platelets during treatment.
Patient outcome
The patient did well and was discharged to rehab on hospital day 23. Patient required multiple orthopedic interventions for her fractures.
Considerations
This was Dr. Vogel’s first deployment and use of the ER-REBOA™ Catheter. Dr. Vogel had taken a REBOA course entitled “Advance Endovascular Skills for Trauma Surgeons” with Dr. Charles Fox from Denver General. As a result of her attendance at this course, Dr. Vogel was asked to present a talk about the ER-REBOA™ Catheter at a trauma nurse symposium the day prior to this patient’s crash. The lecture was a nice refresher and it helped Dr. Vogel and her team become more familiar with REBOA.
Takeaway points:
- Stay calm.
- If access is not easily obtained on one side, go to the other side.
- Prepare REBOA kits and become familiar with their location within the hospital.
- Consider adding extra sheaths and wires in REBOA kits (after this case, it was realized that these extra supplies may be needed).
“I was frankly astonished by the effectiveness and will definitely plan to use the REBOA again,” Dr. Vogel said. “It is very intuitive to place. A patient like this would generally have had an exploratory laparotomy and pelvic packing. A 21-year-old female was spared a large incision that ultimately would have accomplished the same end as a femoral puncture and REBOA placement.”
References:
1. Prytime website / package insert.
2. Moore LJ, Martin CD, Harvin JA, Wade CE, Holcomb JB. Resuscitative endovascular balloon occlusion of the aorta for control of noncompressible truncal hemorrhage in the abdomen and pelvis. Am J Surg. 2016 Dec;212(6):1222-1230.
3. Costantini TW, Coimbra R, Holcomb JB, Podbielski JM, Catalano R, Blackburn A, Scalea TM, Stein DM, Williams L, Conflitti J, Keeney S, Suleiman G, Zhou T, Sperry J, Skiada D, Inaba K, Williams BH, Minei JP, Privette A, Mackersie RC, Robinson BR, Moore FO; AAST Pelvic Fracture Study Group. Current management of hemorrhage from severe pelvic fractures: Results of an American Association for the Surgery of Trauma multi-institutional trial. J Trauma Acute Care Surg. 2016 May;80(5):717-23; discussion 723-5.
4. DuBose JJ, Scalea TM, Brenner M, Skiada D, Inaba K, Cannon J, Moore L, Holcomb J, Turay D, Arbabi CN, Kirkpatrick A, Xiao J, Skarupa D, Poulin N; AAST AORTA Study Group. The AAST prospective Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry: Data on contemporary utilization and outcomes of aortic occlusion and resuscitative balloon occlusion of the aorta (REBOA). J Trauma Acute Care Surg. 2016 Sep;81(3):409-19.

2 Comments
Good Morning. I find the REBOA catheter very interesting. My name is Dr. Homero Zapata Chavira and I work at the University Hospital of Monterrey Mexico, a level I trauma hospital, the most active in the city. We would like to use your catheter, we ask for prices and information to get it.
Thanks for the comment, Dr. Zapata Chavira. I suggest you visit the Prytime website at http://prytimemedical.com/ and click the “Contact us” tab.