
Trauma centers and surgeons are increasingly using REBOA (or resuscitative endovascular balloon occlusion of the aorta) to treat patients in hemorrhagic shock. REBOA isn’t exactly a new procedure. In fact, it’s been around for a while. As noted by Stannard, Eliason and Rasmussen in their 2011 paper in the Journal of Trauma, balloon occlusion of the aorta had its early origins as far back as the Korean War.
But while REBOA is a potentially lifesaving technique, it has not been captured appropriately in many trauma registries. The problem? Limitations of the International Classification of Diseases, 9th Revision, Procedure Coding System (ICD-9-PCS) made it difficult to accurately code this endovascular procedure.
Under ICD-9-PCS, the only code available to use for REBOA was 39.78 — or “Endovascular implantation of branching or fenestrated graft(s) in aorta”.
Fortunately, the recent transition to ICD-10-PCS introduced modifications that now come closer to more accurately describing the REBOA procedure. Any trauma registrar faced with the challenge of abstracting a REBOA case should understand the structure and rationale for these new codes.
Knowing anatomy is key
The first step is to understand how REBOA is currently used. As described by Stannard et al., the REBOA balloon is deployed in one of three “zones” of the aorta [1]:
- Zone I: the descending thoracic aorta between the origin of the left subclavian and the celiac arteries
- Zone II: the paravisceral aorta between the celiac and the lowest renal artery
- Zone III: the infrarenal abdominal aorta between the lowest renal artery and the aortic bifurcation
It’s important to know these zones so one can code appropriately.
The correct codes are available in the 2018 ICD-10-PCS Code Tables and Index provided by the Centers for Medicare & Medicaid Services. (To access this document, visit the “2018 ICD-10 PCS and GEMs” page on CMS.gov and select the correct download.)
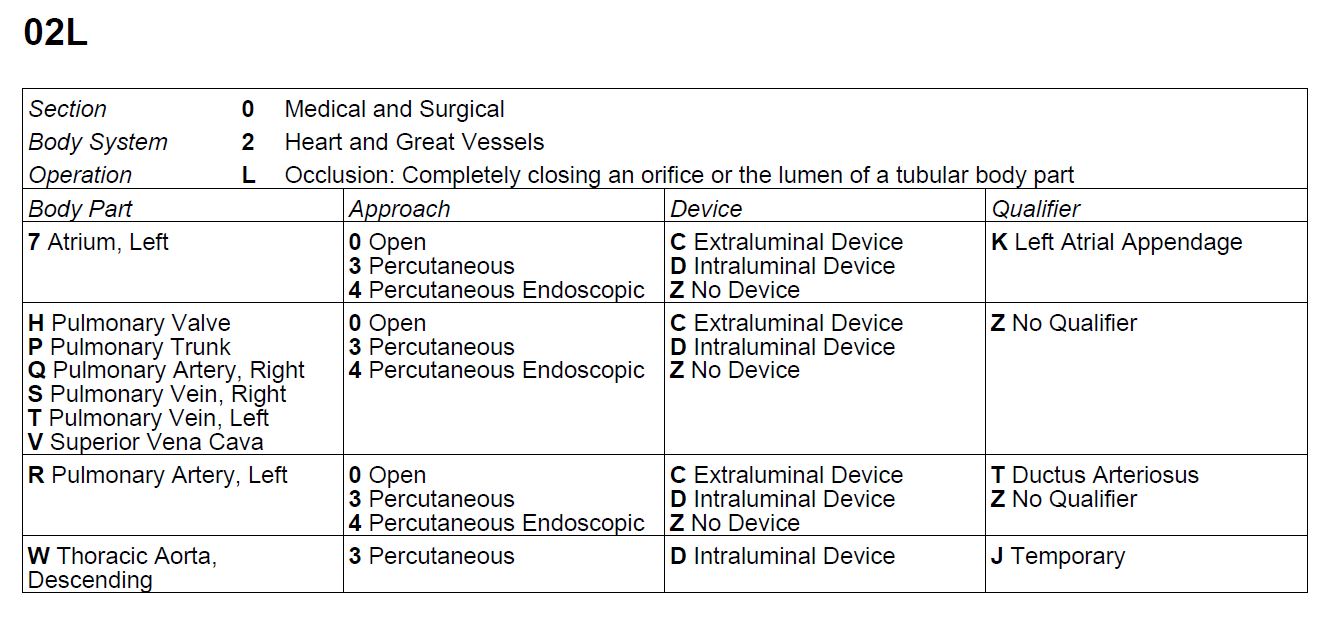
To code Zone I REBOA, use PCS table 02L. This table for occlusion of the heart and great vessels now includes a body part character for “Thoracic Aorta, Descending” and a qualifier character for “Temporary” (see Figure 1).
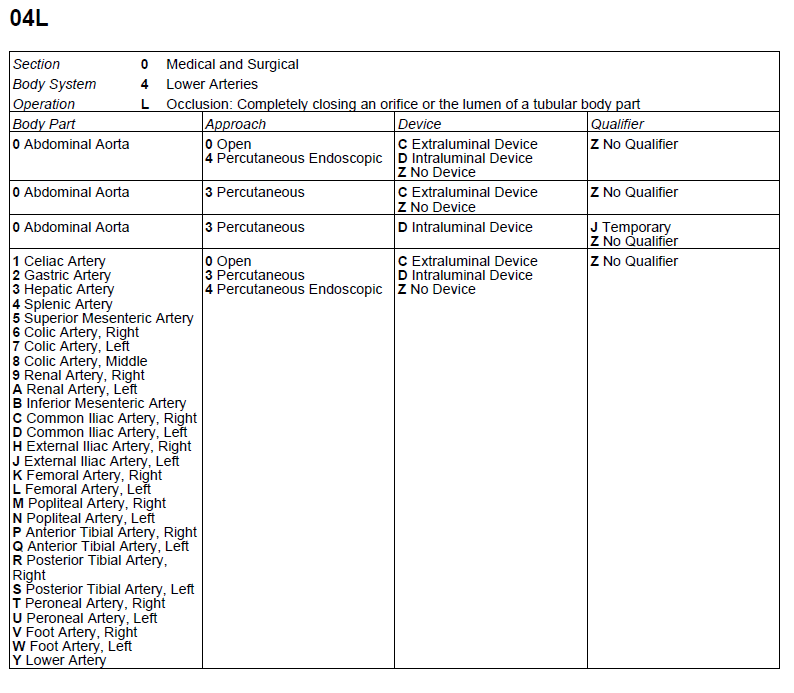
To code Zone II or Zone III REBOA, use PCS table 04L. This table also includes a new qualifier character for “Temporary” for occlusion of the abdominal aorta (see Figure 2).
Keep moving forward
While the current coding tools for REBOA are not perfect, they represent a big improvement over the codes we previously had to use, thus minimizing the effects of the old adage: “Ask five coders the same question, and you will get five different answers.”
For trauma registrars, the keys to success are access to good documentation and personal dedication to ongoing education. As endovascular procedures become more technical, it is important to understand exactly what is being done, how it is being done and why a particular procedure was chosen.
Sandra Strack Arabian MBA, NREMT, CSTR, CAISS is the trauma program manager at Tufts Medical Center in Boston.
References
1. Stannard A, Eliason JL, Rasmussen TE. Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) as an Adjunct for Hemorrhagic Shock. The Journal of Trauma: Injury, Infection, and Critical Care. 2011;71(6):1869-1872. doi:10.1097/ta.0b013e31823fe90c.
2 Comments
Trauma Registry coding of reboa: the ACS has requested that all reboa procedures are to be coded as 04L03DZ, see page 80 of the 2018 dictionary.
Hello,
The code for thoracic aorta was only added for 2018, so indeed, this is an example of the ACS data dictionary needing to clarify further. My humble assumption is that the time in which the data dictionary was written for 2018 (most likely in 2017) I’m sure did not reflect that change in the CMS PCS codes for 2018. So, the philosophical question is If surgeons are using REBOA in Zone 1 why would the registrar code incorrectly thus resulting in the aggregated data NOT reflecting appropriate procedural location? The COT / TQIP needs to weigh in. Thank you for pointing this out.