
Resuscitative endovascular balloon occlusion of the aorta (REBOA) has undergone a renaissance in recent years. Technological advances have turned REBOA into a viable option for many patients with uncontrolled bleeding. As a result, use of the procedure is growing rapidly.
Yet REBOA remains a challenging procedure with significant potential for serious complications. As interest in this intervention grows, some experts worry about a critical skills gap. According to a recent paper in the Journal of Trauma and Acute Care Surgery, REBOA is increasingly performed by physicians who have limited experience with endovascular interventions.
“Most trauma surgeons have no formal endovascular training, other than what they learned as residents during their vascular surgery rotations,” said Megan Brenner, MD, MS.
Unfortunately, current practice may or may not fill the gap for these physicians. “Some trauma and acute care surgeons are routinely involved in procedures requiring vascular access, such as placing catheters for resuscitation, monitoring, ECMO, etc.,” Dr. Brenner said. “But other surgeons are not actively involved in these procedures and have not been in decades.”
For trauma surgeons who are interested in performing REBOA but who need to upgrade their endovascular skills, one solution is simulation-based training. The Mentice endovascular simulation system lets surgeons learn key aspects of REBOA in a risk-free setting.
“REBOA is a new technique performed by providers with variable endovascular skills, and the procedure is not without risk,” Dr. Brenner said.
As described in a study published in the Journal of Trauma, the Mentice simulation model can help physicians improve their knowledge of REBOA and reduce procedural task times, regardless of previous endovascular training.
Learn REBOA on “real” patients
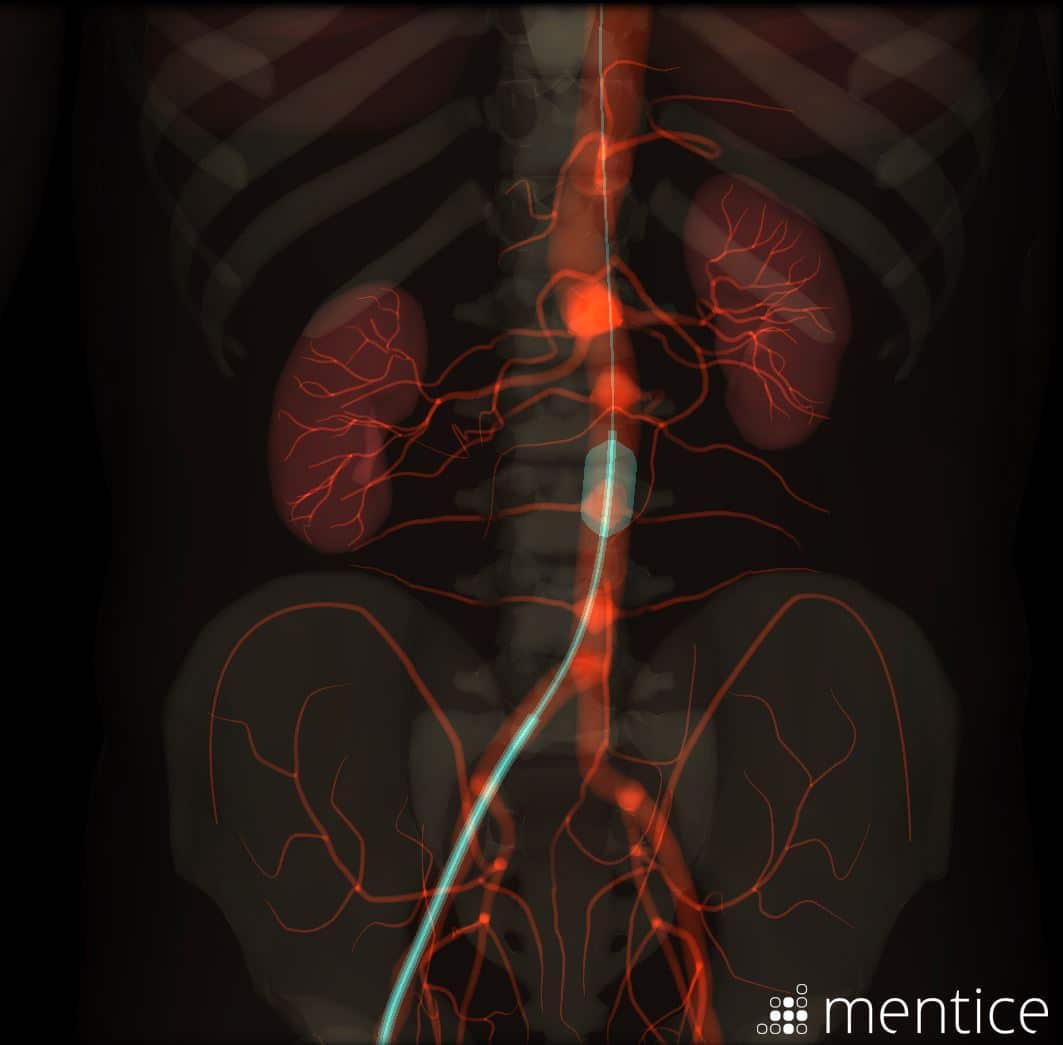
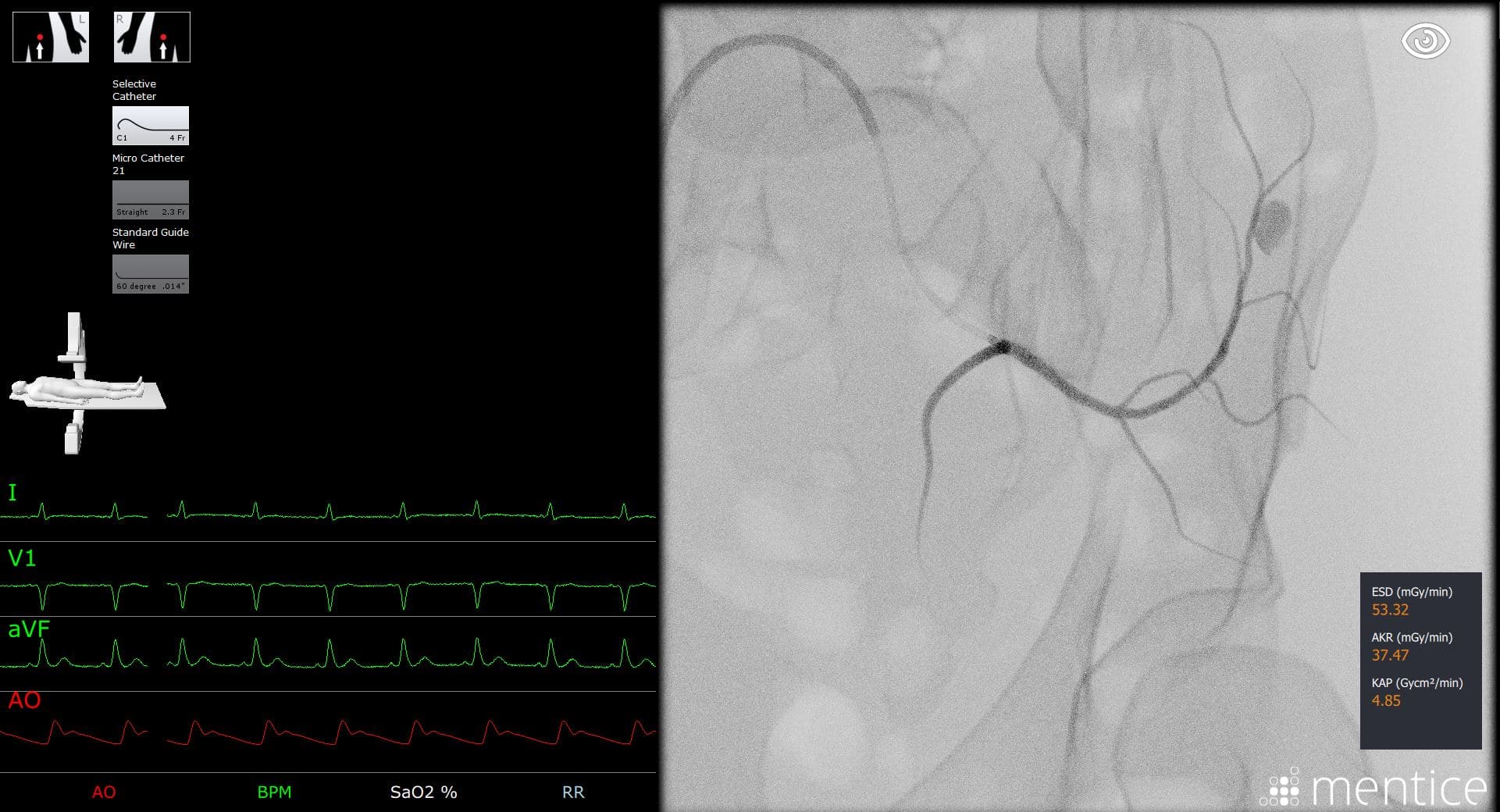
Mentice is a computer-based simulation system designed specifically for training in endovascular procedures. Its Vascular Trauma Management module allows users to learn and practice a variety of trauma interventions using “live” imaging derived from real patient studies.
Trauma surgeons can use the system to learn endovascular techniques for temporizing hemorrhagic shock. Within the simulation, users choose the appropriate endovascular device, practice endovascular manipulation skills, explore various balloon placements, and monitor occlusion via interactive hemodynamics and vital signs.
“After you learn the steps of REBOA, you can use the Mentice system to practice different zone placements and explore different clinical scenarios,” said Ben Speich, director of global operations. “For example, the module includes a variety of pelvic anatomies with multiple bleed sites.”
Mentice is the only computer-based system that simulates the ER-REBOA device. The system provides accurate visual and tactile feedback, creating a realistic experience of performing REBOA and other trauma procedures under X-ray or fluoroscopic guidance.
“With a real patient, you can’t open the abdomen to see where the balloon is,” Speich said. “The Mentice simulator lets you practice manipulating the balloon while you watch it on a monitor. And since the system is X-ray-free, you can practice and experiment with REBOA as much as you like with no radiation exposure to anyone.”
See how to avoid complications
Simulation is an effective element of a REBOA training program. According to Dr. Brenner, many learners also benefit from practicing arterial access in a cadaver lab. “Open surgical femoral artery access is not an intuitive or routine skill for most trauma surgeons,” she said. “That’s why cadaver-based training is important for students who are not comfortable with femoral artery access or arteriotomy repair.”
Dr. Brenner believes simulation training and cadaver-based training are complementary. “Everyone learns at a different pace and takes away different pearls from different simulator experiences,” she said, “so using more than one training modality can be very beneficial.”
No matter what learning modality is in play, training must help learners understand and anticipate the various complications that may arise during different steps of REBOA.
The Mentice system can help trauma surgeons recognize and avoid pitfalls in balloon positioning, balloon inflation and patient management during balloon deployment. For example, the system accurately simulates the arterial injury that can occur when the REBOA balloon is deployed in the wrong anatomical location. In addition, users learn how correct balloon alignment is essential to avoiding small vessel vasospasms and preserving circulation in adjacent vessel branches.
The Vascular Trauma Management module also includes embolization scenarios. Trauma surgeons can team with interventionalists to practice emergency decision making skills and explore multidisciplinary techniques for controlling internal hemorrhage.
Essential for low-volume, high-risk procedures
Even the busiest Level I trauma centers may see only a handful of REBOA-eligible patients per month. At most other hospitals, trauma surgeons will have even fewer opportunities to perform this procedure. Simulation-based training can help trauma teams master this high-risk intervention regardless of REBOA patient volumes.
“As with any procedure, REBOA has a learning curve,” said Göran Malmberg, CEO of Mentice. “At the same time, skills can deteriorate rapidly in the absence of use. High-fidelity simulation allows physicians to train to proficiency in a low-risk setting and then maintain their skills through ongoing practice.”
REBOA remains controversial. Does it make sense for “REBOA skeptics” to train to perform this procedure?
“There is always value in learning more about REBOA,” Dr. Brenner said. “Some people who take the time to learn about REBOA realize that they were skeptical because they didn’t fully understand the procedure or they didn’t see how it could be incorporated into clinical practice at their institution.”
Others are skeptical because there is no definitive high-level data supporting the procedure. “That is absolutely correct,” Dr. Brenner said. “But waiting until we have that data could take years, and being able to use this technique now could help save a patient’s life.”
By learning more about REBOA and training to perform it, all trauma surgeons can contribute to a better understanding of the procedure and how it may or may not benefit patients.
“I always encourage skeptics to learn more about REBOA,” Dr. Brenner said, “since it is through vigorous and critical discussions that we come up with ways to improve the technique and obtain the data that can help guide our clinical use.”
To learn more about the REBOA simulation system available from Mentice, visit the company’s Vascular Trauma Management page.
