
When interest in REBOA was reignited a decade ago, most physicians saw it primarily as an alternative to resuscitative thoracotomy. But according to a group of trauma surgeons in Maine, resuscitative endovascular balloon occlusion of the aorta is actually a versatile tool that can improve patient care in many lower-acuity scenarios.
“Emergency thoracotomy is a very large event with high morbidity and mortality, and unfortunately people tend to view REBOA in a similar light,” said Forest Sheppard, MD, critical care surgeon at Maine Medical Center. “They think of REBOA strictly in terms of putting the balloon up in Zone III for a pelvic fracture or in Zone I for an abdominal hemorrhage.”
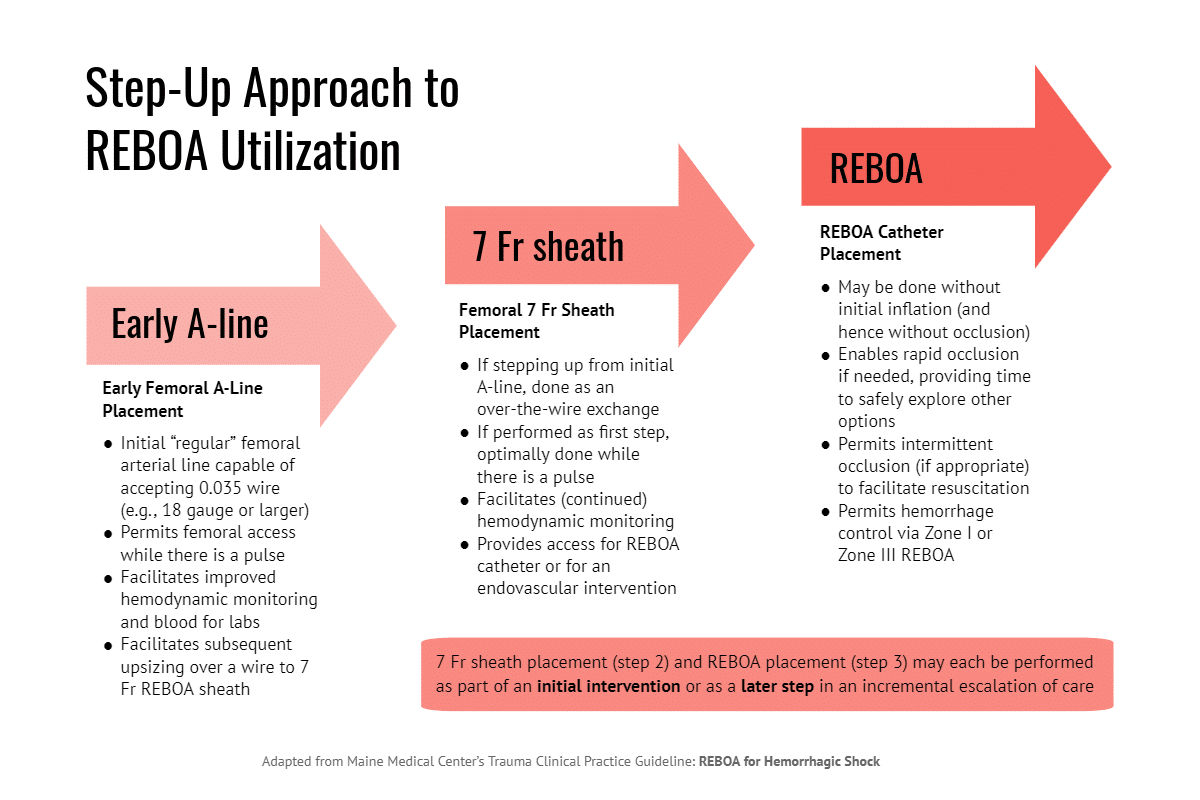
In contrast, Dr. Sheppard and his colleagues view REBOA as a “spectrum of technologies” that can be deployed incrementally in a wide range of clinical scenarios. The spectrum encompasses not just the ER-REBOA™ Catheter, but early femoral artery access and the arterial 7 French sheath. Each technology delivers distinct benefits, and the catheter itself can be used in several ways.
“REBOA is more than just a single procedure for major truncal bleeding,” Dr. Sheppard said. “It is a spectrum of technologies that can be deployed in a very safe and organized fashion to improve patient outcomes at multiple points of care.”
Preserve your options, get access early
The trauma team at Maine Medical Center calls this approach “Step-Up REBOA.” They recently described their strategy in a paper published in Trauma Surgery & Acute Care Open.
According to Dr. Sheppard, the starting point of Step-Up REBOA is early access to the common femoral artery. “Beginning with good arterial access allows improved physiologic monitoring and it also lets you ‘get your foot in the door’ in case you need to escalate care.”
The next level of care is introduction of the 7 Fr vascular sheath, but this step is not just the gateway to catheter placement. “The vascular introducer sheath can be used for either continued hemodynamic monitoring or, potentially, an intravascular intervention.”
Step-Up REBOA can improve care in several ways, even if the surgeon never escalates to the catheter itself. As described in the Maine team’s recent paper, one of the first cases to inform this approach was an adult male who presented with right flank pain following a bicycle crash.
“The patient’s initial systolic blood pressure was below 90 mmHg, and he had a grade 5 kidney laceration on CT,” Dr. Sheppard said. “We were anticipating a difficult surgical repair and possible nephrectomy, so we obtained CFA access and placed a 7 Fr introducer sheath to enable fast aortic occlusion if needed.”
Once the A-line was placed, however, invasive monitoring showed SPB of 110. With hemodynamic stability confirmed and rapid occlusion possible if the patient’s condition worsened, the team had time to explore other options. Ultimately, an interventional radiologist performed a renal artery embolization through the introducer sheath.
Dr. Sheppard noted that early arterial access alone provided important data that improved clinical decision making. In addition, placing the introducer sheath facilitated rapid definitive care via an IR procedure.
“It gave us the chance to rethink our plan because I knew that at any moment I could put up the balloon and stop all hemorrhage,” he said. “That gave us the opportunity to go in a different direction that really worked out very well for the patient.”
A versatile tool
For cases that do escalate to catheter deployment, the step-up strategy views ER-REBOA™ as a versatile tool that can be used in different ways.
Another patient described in the team’s recent paper was a 60-year-old female with hemodynamic instability following a motor vehicle crash. After her second traumatic arrest, the team deployed the ER-REBOA™ Catheter to Zone III and used aortic occlusion intermittently to divert circulating blood volume to the heart, lungs and brain.
“This strategy stabilized the patient sufficiently to avoid immediate transfer to the OR,” Dr. Sheppard said. “With the catheter in place, we knew we could do resuscitative aortic occlusion as needed, so we took her to CT.”
Imaging showed multiple fractures and other injuries, but no obvious sources of massive bleeding. The patient was transferred to intensive care and was managed successfully with nonoperative means.
“The tone and course of our resuscitation would have been much different if the patient had undergone [resuscitative thoracotomy],” the paper authors wrote. “REBOA allowed us to safely obtain imaging information that steered us toward the ICU and controlled resuscitation and away from surgery which would not have found an obvious source for her hemorrhagic shock. The REBOA system was used not as a bridge to surgery, but as an adjunct to hemostatic resuscitation[.]”
Indications for Step-Up REBOA
According to Bryan Morse, MD, a member of the Maine trauma team, Step-Up REBOA should be initiated for all patients at high risk for needing an aggressive resuscitation.

“When you don’t know a patient’s physiologic status right off the bat but you get a sense that they have critical injuries due to low first blood pressure or high shock index, you want to go ahead and get that A-line in early,” Dr. Morse said.
Under the team’s clinical practice guideline, the main indications for early arterial access are initial SBP under 100, shock index greater than 0.9 or change in shock index of 0.3 or more. (For Maine Medical Center’s complete Step-Up REBOA guideline, see the “supplementary data” section of ‘Step Up’ approach to the application of REBOA technology in a rural trauma system.)
Maine Medical Center, a Level I trauma center, is working with hospitals throughout the state to implement Step-Up REBOA as a regional strategy. “In this state, the transfer time to our center can be anywhere from one hour up to 10 hours, so we are very interested in involving outside hospitals in the step-up approach,” Dr. Morse said.
“If physicians in rural Maine can get early arterial access, they can get good physiologic data and relay that information to us,” he said. “We can then help them decide on next steps, whether the patient would benefit from blood before transfer, air evacuation, some other intervention, or ultimately REBOA.”
Monitoring Step-Up REBOA for quality and safety
The Maine team’s Step-Up REBOA guideline includes several protocols for monitoring femoral sheaths and catheters in intensive care. In addition, all trauma patients cared for under the step-up guideline go through the program’s performance improvement (PI) process.
“We peer review every access, sheath placement and catheter deployment,” Dr. Morse said. “Obviously, we are looking at mortality and complications but also time to access and time to placement, because that’s an important question for trauma surgeons: Am I spending time getting this catheter in that I should have spent getting the patient to the OR?”
According to Dr. Sheppard, the PI program also monitors comparable cases in which Step-Up REBOA was not used. “These are cases where following the step-up approach might have avoided a delay in diagnosis or a delay in care.”
Not “all or none”
The key to implementing a step-up strategy is to gain a better appreciation for how the ER-REBOA™ can be used incrementally.
“I think that so many things we do in medicine are ‘all or none’,” Dr. Sheppard said. “For example, you either put in a chest tube or you don’t, but you never put it in halfway.”
“The idea we are trying to develop here is that REBOA is not an ‘all or none’ phenomenon but a spectrum of technologies that you can escalate as needed,” Dr. Sheppard said. “You might go all the way up to occlusion, but the step-up strategy also gives you the opportunity to improve care even if you never go beyond the A-line.”
