
Trauma resuscitation has changed a lot in the last 20 years. Not that long ago, most hemorrhagic shock patients received a crystalloid-based resuscitation. Many of us remember the resulting open abdomens with planned ventral hernias. That paradigm eventually gave way to blood component therapy with balanced ratios, followed by the goal of limiting crystalloids altogether while targeting 1:1:1. Today, we are all beginning to appreciate the benefits of whole blood in trauma resuscitation.

Whole blood has the advantage of obviating the need for components, at least in the beginning of a massive resuscitation. However, it creates a fresh logistical challenge for civilian trauma centers that are geared for component therapy.
How do we secure a stable supply of whole blood while minimizing waste? How do we coordinate whole blood with our existing component therapy protocols? How does a whole blood program at one trauma center fit into the regional trauma system?
These are just a few issues that need to be addressed by any trauma leader interested in whole blood resuscitation. In this article, I will try to shed light on these issues by outlining five questions you need to answer when you are designing a whole blood program.
Full disclosure: I have no special qualification in transfusion medicine. But I have set up whole blood programs for trauma. In the process, I learned a few principles about blood management that might help others.
1. What is the logistics of our blood supply?
Whole blood (WB) has a shelf life of 21 days. Any unused units should be returned before the expiration date because expiring blood can be spun down to its components so the blood is not wasted. The hospital will typically receive credit for the returned units, which helps control hospital costs.
However, it is important to understand where your hospital’s blood comes from. Not all blood banks are equal. Most are simply centers for storing and distributing blood products. A smaller number of blood banks are designated as blood processing centers. Whether you are supplied by a regular blood bank or a blood processing center will have a big impact on the logistics and costs of your WB program.
- If your hospital is supplied by a blood processing center, you can return unused whole blood shortly before the expiration date.
- However, if your hospital is supplied by a regular blood bank, you need to build in additional time for travel and processing.
At the trauma center where I created a WB program, the blood supplier was a regular blood bank without processing capabilities — so we needed to return unused WB units to the regional blood processing center. However, the courier between the hospital and the processing center ran only twice a week. After accounting for delivery time and other logistical issues, the effective shelf life of our whole blood was actually just short of 14 days.
As a side note, it is useful to understand that most of the trauma centers pioneering the whole blood movement actually own their own blood processing center. This simplifies logistics and helps ensure they can run a WB program with very little waste.
I am not saying that a hospital must own a blood processing center in order to make whole blood practical. The point is simply that supply is a critical success factor, and trauma leaders that want to use whole blood need to carefully manage blood logistics.
2. How will we pay for our whole blood program?
How does whole blood compare to packed red blood cells (PRBCs) in terms of cost? You will need to find out from your blood supplier, but I recommend coming to the discussion informed.
When I first asked about setting up a WB program, I was told that it would be cripplingly expensive. However, it turned out that whole blood was actually cheaper than component therapy. In our experience, each unit of whole blood is a little more expensive than a unit of PRBC — but much less expensive than a unit of PRBC plus a unit of fresh frozen plasma (FFP).
Again, talk to your blood supplier to understand the costs of WB, PRBC, FFP and other components. After you do your homework, create a pro forma financial statement for your WB program. Key assumptions may include patient volume and projected WB utilization. The pro forma should also include wastage. Attention to logistics (see above) will help you minimize waste as much as possible, but some wastage is unavoidable, particularly for low-volume centers.
The pro forma will provide the cost justification when you seek approval for your WB program. Depending on how your hospital agreements are structured, you will need to gain approval from either the trauma multidisciplinary committee and/or the blood bank.
3. How exactly will we use whole blood in our trauma program?
The basics of whole blood transfusion are well known:
- Patients at most adult centers must be at least 12 years old
- Males receive type O+
- Females over 60 receive type O+
- Females 60 or younger receive type O-
Titer levels represent the amount of antibodies present in the whole blood that could cause a reaction. There is a lot of debate about titers, but most WB programs use blood that is less than 50 titers. Type O blood under 50 titers can be given to most patients with low likelihood of a reaction. It is worth noting that some places, such as Norway, use zero titer whole blood.
How much whole blood should you have on hand and how should you use it? The most common approach is to stock 2 units of O- whole blood and 2 units O+ whole blood in a trauma bay refrigerator. A patient in need of blood transfusion starts with 2 units of whole blood. After that, switch to MTP component resuscitation.
4. What is our lab’s policy for patients who receive whole blood?
 If you are going to give patients whole blood, you will need to monitor them for adverse reactions. In my experience, this is the most variable policy between different trauma centers. Some hospitals draw labs before transfusion and again at 24 or 48 hours. Others do not have any policy on WB lab tests, which means that trauma will be the driving force for creating one.
If you are going to give patients whole blood, you will need to monitor them for adverse reactions. In my experience, this is the most variable policy between different trauma centers. Some hospitals draw labs before transfusion and again at 24 or 48 hours. Others do not have any policy on WB lab tests, which means that trauma will be the driving force for creating one.
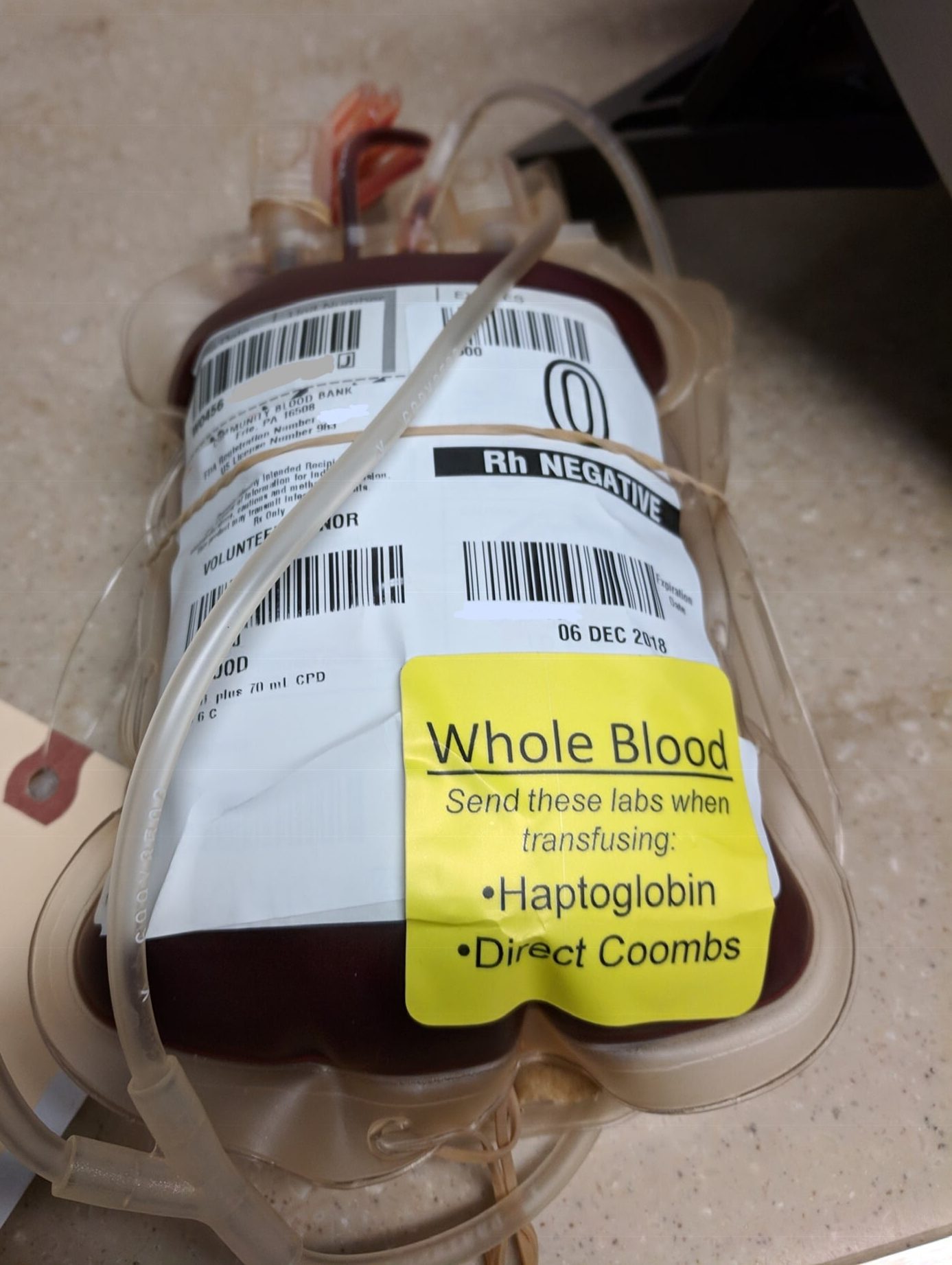
The first step, of course, is to consult your hospital protocols. You should also check with your blood supplier for any lab requirements. A common and very conservative approach is to draw a direct Coombs test and a haptoglobin test at baseline (before transfusion) and again at 48 hours.
As everyone knows, it can be difficult to remember to send these labs during the chaos of a trauma resuscitation. One solution is to affix large yellow reminder stickers to each unit of whole blood: “Send these labs before hanging whole blood.”
5. How does whole blood affect patient transfers?
What will happen when a patient receives whole blood in your hospital and is then transferred to another hospital?
This is a very important question to answer if you might be transferring patients to a hospital that does not use whole blood. I recommend meeting with the trauma medical director of any receiving hospital. Inform the TMD about your new WB program and discuss lab and follow-up protocols.
It is also important to create a process for alerting staff at the receiving hospital that a whole blood patient has arrived. The simplest approach is to make sure this information is included in the physician-to-physician sign-out.
Alex Guerrero, MD, MSc, FACS is a trauma surgeon based in New York City. He is the founder of InterTrauma.