
Is a child’s airway the same as an adult’s, only smaller? The answer is “yes and no.” The anatomical structures of the adult and pediatric airways are the same. However, pediatric airway structures are not only smaller but less developed. This creates several specific challenges to airway management.
Trauma nurses should understand the unique challenges to maintaining a patent airway in a pediatric patient. They should also recognize the often subtle signs of airway compromise in infants and children.
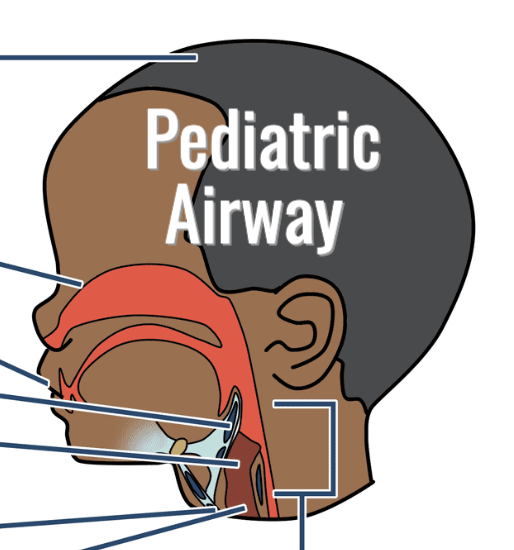
Q. What are the main differences between the pediatric airway and the adult airway?
There are several anatomic and physiologic differences between adult and child/infant airway structures that can affect the care and management of the pediatric trauma patient.
Risk of neck flexion. An infant or small child has a relatively large occiput (the back of the skull) in comparison to an adult. This increases the risk of neck flexion when the child is laying supine.
Infants have low tolerance of nasal obstruction. Infants have relatively narrow nasal passages. Since they are nose breathers, they are less able to tolerate nasal congestion or obstruction.
Infants have increased risk of tongue obstruction. Infants have relatively small mouths. As a result, the infant’s tongue and soft tissue fill the mouth, increasing the risk of tongue obstruction.
Differences in the epiglottis. The adult epiglottis is relatively wide and more horizontal. The infant epiglottis is narrower, more vertical and more anterior. The epiglottis in a small child is large and floppy.
Differences in the larynx. Adults have a cylinder-shaped larynx. In contrast, infants and small children have a funnel-shaped larynx.
Higher risk of mainstem intubation. The trachea of an infant or small child is relatively narrow and short compared to an adult trachea. This increases the risk of a right mainstem intubation.
Relatively small cricoid membrane in infants and small children can make needle cricothyroidotomy more challenging.
Relatively narrow bronchi and bronchioles in infants and small children can increase airflow resistance.
No identifiable oropharynx in infants and a small oropharynx in young children means the pediatric airway can easily become obstructed by the large tongue.
Q. What are the signs of airway compromise in a pediatric patient?
Trauma nurses should watch pediatric patients for several signs and symptoms of possible airway obstruction.
Signs of UPPER airway obstruction:
- Stridor (noisy high-pitched breath sounds)
- Hoarseness
- Weak cry or change in cry
- Inability to vocalize or change in voice
- Inspiratory retractions (on inhale, skin between the ribs or in the neck sinks in)
- Nasal flaring
- Increased respiratory rate and effort
- Poor chest expansion
- Drooling, gurgling or snoring
- Poor air entry on auscultation
Signs of LOWER airway obstruction:
- Increased respiratory rate
- Wheezing
- Decreased air entry on auscultation
- Cough
Q. What non-invasive maneuvers can help open the pediatric airway?
Trauma nurses can attempt to open up the child or infant airway with some non-invasive positioning maneuvers.
Place the child in the sniffing position. Position the child with the neck flexed forward at the shoulder level (but not hyperextended) and the head extended. (Think of the way you lean forward to smell a rose — not overextended but chin up and head slightly forward.) You may need to place a folded towel or blanket under the shoulders to accommodate the large occiput.
Let the child assume a position of comfort. If the child is awake, allow him or her to assume a position of comfort that facilitates breathing (for example, the tripod position). Do not force a child to lie supine if it makes him or her uncomfortable or negatively affects the ability to breathe.
If NO cervical spine injury is suspected, perform the head tilt/chin lift. Push down on the forehead to tilt the child’s head back. Place one or two fingers under the patient’s chin bone and pull up.
If cervical spine injury IS suspected, perform the jaw thrust maneuver. Stand at the patient’s head and slide one hand under each angle of the mandible. Pull the jaw upward and outward to prevent the tongue from obstructing the airway.
Q. What other basic interventions can be used to open the pediatric airway?
Suctioning. If the oral airway is compromised by liquids such as blood, vomit or secretions, you can use a semi-rigid oropharyngeal suction catheter (tonsil tip) to clear the oropharynx. (Be careful not to suction too aggressively or deeply — vagal stimulation may cause bradycardia.) If the nasal airway is compromised, use a soft suction catheter to clear the nasopharynx. For newborns or infants, you can use a bulb syringe to clear nasal or oral secretions.
Airway insertion. If an unconscious or semi-conscious infant or child cannot effectively protect their airway, you can insert an oral or nasal airway. For unconscious infants or children without a gag reflex, insert an oropharyngeal airway as a temporary measure until a definitive airway can be placed. For unconscious or semi-conscious infants or children without facial trauma, suspected facial fractures or suspected head injury, insert a nasopharyngeal airway.
Learn more about the pediatric trauma patient
This article is based on Pediatric Emergency Airway Management, an interactive online course from the Board of Certification for Emergency Nursing (BCEN®). Developed by trauma nursing experts, this CE-eligible course teaches nurses how to quickly recognize airway compromise in the pediatric patient and initiate timely, lifesaving interventions. To access Pediatric Emergency Airway Management and other courses for trauma nurses, visit BCEN Learn.
![]() Pediatric Emergency Airway Management supports the continuing education requirements of the Trauma Certified Registered Nurse (TCRN®) program. The TCRN credential is the only national board certification for trauma nursing, and it spans the body of knowledge for care of the injured patient. Approximately 8,500 nurses worldwide have earned the TCRN credential. For more information, click here.
Pediatric Emergency Airway Management supports the continuing education requirements of the Trauma Certified Registered Nurse (TCRN®) program. The TCRN credential is the only national board certification for trauma nursing, and it spans the body of knowledge for care of the injured patient. Approximately 8,500 nurses worldwide have earned the TCRN credential. For more information, click here.