
Most trauma program leaders are familiar with the Plan-Do-Study-Act (PDSA) model for healthcare improvement.
However, while almost everyone understands the basic concept, many trauma program teams are unclear about when to use the PDSA model and when another approach is indicated.
The goal of this article is to explain PDSA’s role in trauma performance improvement by showing how it was applied in an actual clinical setting.
This example is based on a recent PI project at NYC Health + Hospitals/Jacobi, a Level I adult and Level II pediatric trauma center in New York City. This project focused on improving care for patients with suspected acute compartment syndrome.
The problem of acute compartment syndrome in trauma
To review, acute compartment syndrome is a surgical emergency caused by a rapid increase in pressure within a muscle compartment. This pressure increase restricts blood flow, leading to ischemia and ultimately tissue death.

In trauma, acute compartment syndrome is most common in the anterior compartment of the lower leg. However, it can arise in any muscle compartment enclosed by rigid fascia: thigh, foot, forearm, hand, gluteal region, abdomen, etc.
Traditionally, compartment syndrome is diagnosed by the “six P’s” — pain, paresthesia (tingling sensation or numbness), pulselessness, poikilothermia (inability to maintain a constant core temperature), paralysis and pallor.
The challenge is that pain is a non-specific sign. Especially in the setting of trauma, pain can be caused by many different issues. And the remaining five P’s are all late signs. They usually appear only after irreversible damage has occurred.
In practice, this diagnostic uncertainty creates a high risk of both overtreatment (unnecessary fasciotomy) and undertreatment (delayed care leading to muscle death or amputation).
This is not just a theoretical problem. According to data from the Trauma Quality Improvement Program (TQIP), the national fasciotomy rate is four times the true incidence of compartment syndrome.
Why PDSA is right for this issue
Before we get into the details of this project, let’s take a step back and look at what’s happening here.
Acute compartment syndrome is a relatively frequent occurrence in trauma, so it’s an urgent problem. At the same time, the proper management of these patients requires the cooperation of several surgical specialties, and it has implications for trauma standards compliance, trauma nursing workflows and even trauma data management. So it’s also a complex problem.
This is exactly the kind of problem that the PDSA model was designed to solve.
PDSA is all about performing iterative cycles of change that are rapid but also carefully designed to yield solid knowledge. So it is perfectly suited for tackling issues that are both urgent and complex.
When you are faced with a problem that is either not urgent or not terribly complicated, the right approach will usually be straightforward corrective action with monitoring compliance.
But if you are faced with an issue that is both high-impact for patients and high-complexity from an implementation standpoint, you need to use a rapid-cycle PDSA.
PLAN a change or improvement
The key to making a PDSA improvement cycle as fast as possible is to make it as focused as possible. That means not just describing the change you want to test but also thinking through the rationale and goals of the entire project.
Here is how the team at Jacobi Medical Center mapped out the plan:
Define the problem. Our problem statement encapsulated the root cause and the impact on patients:
“Current practice patterns show variability in the assessment and diagnosis of acute compartment syndrome, leading to delays in care and fasciotomies that may not be clinically indicated. This variation increases patient risk, resource utilization and downstream complications.”
Formulate the aim. What are you actually trying to improve? The Jacobi team’s aim was both specific and measurable:
“The aim of this project is to reduce delays in care and unnecessary fasciotomies by 25%.”
Design the change. At Jacobi, the core of our intervention was the MY01 Continuous Perfusion Sensing Technology Platform, a device that enables continuous monitoring of pressure within physiological compartments. In addition, key stakeholders revised existing guidelines (see below) and developed new workflows to support this intervention.
DO the improvement (make the change)
The cornerstone of a PDSA execution phase is typically a new or revised clinical practice guideline. At Jacobi, the orthopedic surgery liaison, a trauma surgeon, the TPM and the PI coordinator worked to revise the existing compartment syndrome guideline to include (a) the use of continuous pressure sensor technology and (b) escalation parameters to ensure appropriate and timely interventions.
The staff education plan covered how to identify patients with suspected compartment syndrome, how to use the MY01 device, and how compartmental pressure data fits into the care strategy for these patients. Hands-on education was provided to trauma surgeons, orthopedic surgeons and medical residents, as well as nursing staff in the ED, ICU, OR and PACU.
Critically, the “do” phase also included a plan for capturing and interpreting project data. This plan included:
-

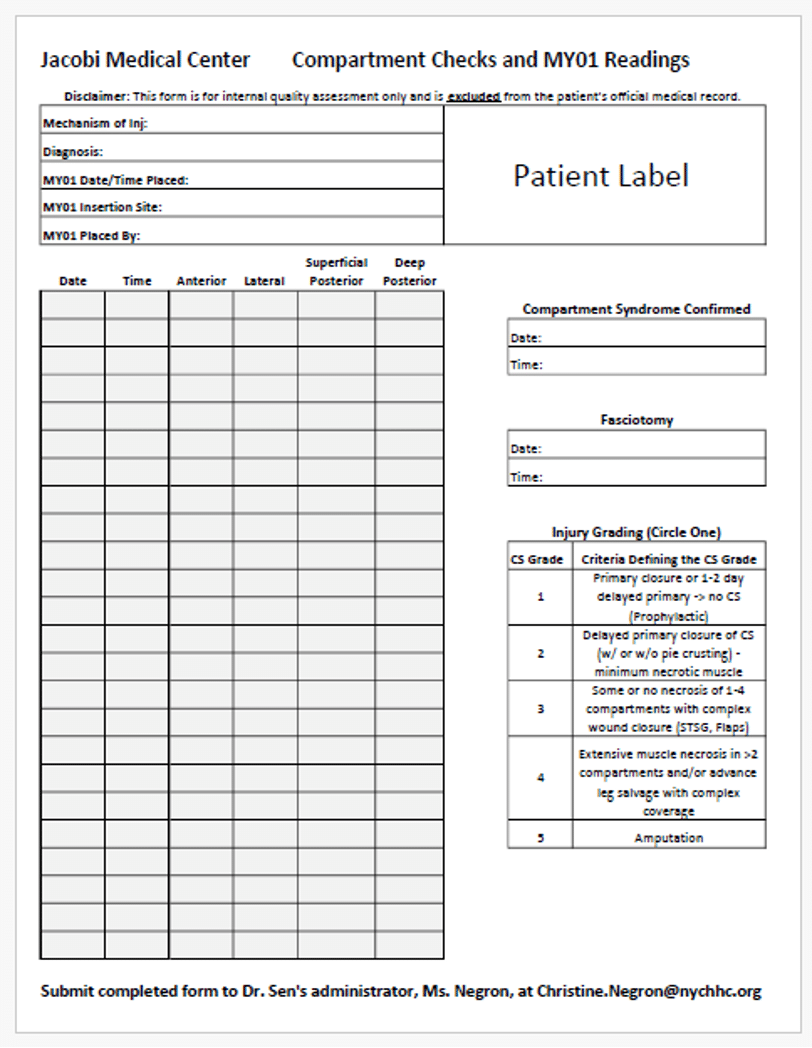
Compartment pressure documentation form (CLICK to enlarge) Creating a documentation tool to capture key information on patients cared for under the project protocol. (Click the thumbnail at right to view the form.)
- Educating trauma registry staff on how to code continuous pressure monitoring in ICD-10.
- Creating an audit filter within the trauma registry that allows users to flag cases involving acute compartment syndrome, enabling easy tracking of cases that fall under the PDSA.
- Adopting a 5-class post-fasciotomy grading system for assessing the effectiveness of monitoring and the timeliness of interventions.
STUDY the results
The key to an effective “study” phase is to select performance measures that can demonstrate whether a change did or did not improve care. At Jacobi, we decided to focus on the incidence of tibia fractures (proximal and shaft) as the denominator, with the incidence of acute compartment syndrome with and without fasciotomy as the numerators. We also considered the incidence of amputation as a signal of a delay in diagnosis.
We monitored our intervention for a period of 10 months, during which 26 patients were identified as having increased risk for developing acute compartment syndrome.
Of these patients, 23 received continuous pressure monitoring and 3 received a clinical exam only. Here is the comparison:
| Continuous pressure monitoring | Clinical exam only | |
| Patients (#) | 23 | 3 |
| Fasciotomy | 10 | 3 |
| No fasciotomy | 13 | 0 |
| Amputation | 0 | 1 |
While the number of patients monitored during this project was small, it was enough to demonstrate the practical value of the new continuous pressure monitoring technology coupled with a clinical practice guideline.
Among the patients managed with clinical signs only, all three received a fasciotomy and one patient underwent an amputation. In comparison, among the group monitored using the MY01 device, more than half avoided fasciotomy and none progressed to limb loss.
(To learn more about this project, view our recent webinar: Compartment Syndrome: Achieving Zero-Miss, Low-Complication Outcomes Through Continuous Monitoring and PI-Driven System Change.)
ACT to sustain performance and spread change
If the study phase of your PDSA shows mixed results, the “act” phase is your opportunity to review what seemed to work well, what fell short and how your team can fine-tune the intervention.
However, even if your PDSA yields strong results in the first cycle, the act phase is not just a victory lap. This crucial step should be a formal effort to sustain the change, spread it to other teams or departments, and maintain ongoing results.
Following the initial cycle of our compartment syndrome PDSA, it became apparent that we needed to adjust our implementation plan to ensure sustainability. To maintain ongoing results at Jacobi, the team:
- Implemented a train-the-trainer model to ensure and spread competency in managing acute compartment syndrome.
- Worked with the hospital’s Epic team to embed standardized documentation tools for compartment syndrome and intracompartmental pressure within the EHR.
- Continued to audit guideline compliance and report variances as they occur.
For trauma program leaders, this model covers the entire cycle of trauma PI, including event identification, corrective action, effective use of audit filters, results sustainability and loop closure — all summarized on one page.
For that reason it is a great way to satisfy ACS Standard 7.3, which requires trauma centers to document the effectiveness of their PI program.
Want to dig deeper on PDSA?
If you would like to learn more about using the PDSA model to address complex issues in trauma quality, I invite you to attend my upcoming “PDSA Workshop for Trauma PI Professionals”.
This workshop will be presented in June in conjunction with the Virtual Summit on Trauma Performance Improvement.
During this workshop, I will drill down on when to use the PDSA, common pitfalls to avoid, how to troubleshoot mixed results and more.
Registration for the workshop will open in May — but if you would like to receive advance notice, I invite you to fill out the “early notification” request below.